
Treatment of Mild to Severe Acne Vulgaris With a 650-Microsecond 1064-nm Nd:YAG Laser
Nazanin Saedi MD, Thomas Griffin Jr MD, Sara Kelly CMA
Dermatology Associates of Plymouth Meeting, Plymouth Meeting, PA
Abstract
Background: Effective treatment of acne remains a challenge to dermatologists.
Objective: To evaluate the efficacy and tolerability of a 650-microsecond, pulsed 1064-nm Nd:YAG laser therapy for mild to severe facial acne vulgaris.
Methods: Human subjects of Fitzpatrick skin types I to VI with mild, moderate, or severe acne enrolled in the prospective, single center study. Subjects received 5 treatments at 2-week intervals with the 650-microsecond, 1064-nm, pulsed Nd:YAG laser. Follow-up visits were 30 days and 90 days after the final treatment. At each visit, subject global assessments, lesion counts, investigator’s global assessments (IGAs), and tolerability appraisals were performed.
Results: The median percent reduction in lesion count was 48.15% after 1 treatment and 83.72% at treatment 3 and remained at 86.67% at 90 days. Sixty percent of subjects noted improvement after treatment 1, and most subjects noticed improvement on or before treatment 3. Median IGA values decreased rapidly to reach a plateau of 1.0 (almost clear) at week 6 and remained there at the 30- and 90-day follow-up. Ninety percent of subjects were slightly to highly satisfied after 3 treatments, and 90% slightly to strongly agreed that their acne treatments improved their self-esteem after 4 treatments. Anesthesia or skin cooling were not used, and adverse events were not observed.
Conclusions: The 650-microsecond, pulsed 1064-nm Nd:YAG laser has been proven to deliver long-lasting clearance of mild to severe facial acne vulgaris with high subject satisfaction and without adverse effects on skin types I to VI.J Drugs Dermatol. 2024;23(11):957-964. doi:10.36849/JDD.8171
Introduction
Acne affects approximately 50 million people in the United States.1 Therapies include retinoids, antibiotics, hormones, lights, lasers, and various combinations of these modailties.2 Topical and/or oral medications are associated with adverse effects, partial response, contraindications, and reoccurrences.3 The advantages and disadvantages of various lasers used alone or in combination with other modalities to treat acne have been described.2 Reluctance to use laser devices historically for acne therapy has included concerns about pigmentary side effects(particularly on Fitzpatrick skin types IV-VI), treatment pain, and low treatment efficacy. A recent review4 reported that high-level studies support the effectiveness of Nd:YAG laser devices compared with other laser devices. The present study evaluates the efficacy and tolerability of a 650-microsecond, pulsed 1064-nm Nd:YAG laser for the treatment of mild to severe facial acne vulgaris.
Materials and Methods
Study Design
Subjects (n=23, aged 29.4 ± 6.7 years [mean ± SD], 20 females and 3 males, Fitzpatrick skin types I-II [35%], III [9%], IV [30%],V[17%], VI [9%]) with mild (4%), moderate (57%), or severe (39%)acne enrolled in the prospective, single-center study. Subjects received 5 treatments at 2-week intervals with the 650-microsecond, 1064-nm, pulsed Nd:YAG laser (Neo Elite, Aerolase Corp., Tarrytown, NY) without topical anesthetic. At visit 1, qualified subjects (n = 20) received a physical exam, dermatological history, and review of concomitant medications. Women of childbearing potential were required to have a negative urine pregnancy test at each treatment visit. Followup visits were 30 days and 90 days after the final treatment. At each visit, photographs, adverse event inquiries, subject global assessments (treatment pain, satisfaction with treatment, post treatment improvement, self-esteem), lesion counts, investigator’s global assessments (IGA), and safety appraisals were performed. Subjects did not use anti-acne prescription or topical OTC medications for 2 weeks prior to or during the study. All subjects provided signed informed consent.
Subjects
Qualified subjects were males or non-pregnant females aged 19 to 40 years with mild to severe facial acne with inflammatory lesions and no more than a single nodule or 2 acne cysts. Exclusions were pregnancy, unwillingness to use an effective method of birth control for women on child-bearing potential, male with facial hair that would interfere with the study, use of topical retinoid within the previous month, use of topical antibiotic within the previous 2 weeks, use of oral antibiotic or isotretinoin within the previous month, participation in another clinical trial in the past 30 days, or presence of a serious medical condition that could put the subject at risk or interfere with interpretation of trial results.
Laser Treatment
Prior to laser treatment, the skin was thoroughly cleaned with alcohol swabs and dried thoroughly. Eye shields were placed over the eyes. Laser treatments were performed in 2 steps. In the first step, the clinician applied 4 passes with the laser over the entire face. Laser settings for each subject were based on the Fitzpatrick skin type, as shown in Table 1.
Table 1

In step 2, as in step 1, settings varied with the subject’s skin type. For skin types I through III, the clinician changed the lens to a 2-mm spot size. Additional pulses were applied only to active acne lesions. Three to 5 pulses were applied to smaller lesions and 5 to 15 pulses to larger nodular/cystic acne lesions; the larger the lesion, the more pulses were applied. Typically, active acne lesions became lighter in color and smaller in size and may have purged sebum.
For skin types IV through VI, settings are shown in Table 2. Three pulses were applied to each smaller lesion and 5 pulses to the larger nodular/cystic acne lesions.
Table 2

Photography
Three digital photographs were taken of each subject at each visit: one at 0° in the front face with the camera within the sagittal plane and two at +45° and -45° in front of the face, respectively, with the camera between the sagittal and coronal planes.
Adverse Events/Safety
Adverse events and safety were monitored at each visit before treatment. Edema, erythema, acne flare-ups, dryness, and itchiness were graded as none, mild, moderate, or severe.
Acne Lesion Count
Acne lesion counts were performed “live” by the investigator(not from a photograph) prior to treatment and included only the active lesions. Inflammatory lesions on the forehead, left cheek, right cheek, nose, and chin were counted, excluding red, brown, or hyperpigmented spots caused by acne.
Investigator’s Global Assessment
The IGA assesses acne severity from 0 to 5, where 0 = clear skin,1 = almost clear, 2 = mild, 3 = moderate, and 4 = severe, and5 = very severe.
Subject Global Assessment
After each treatment, subjects provided feedback on the level of treatment pain on a scale of 1=no pain to 10=intolerable pain. Subject satisfaction with the treatment was assessed on a scale of 1=highly dissatisfied, 2=slightly dissatisfied, 3=neutral,4=slightly satisfied, and 5=highly satisfied. Subjects were asked to specify the treatment (0 [baseline] to treatment 5), after which he or she first noticed an improvement in acne. Subjects were asked to (1) judge the percentage of clearance (0-100%) from when the treatment began and (2) if the treatment improved the subject’s self-esteem, using the scale 1=strongly disagree,2=slightly disagree, 3=neutral, 4=slightly agree and 5=strongly agree.
Table 3
Data Analysis
Data consisted of small whole numbers not normally distributed, as shown by the Shapiro-Wilk test. Nonparametric statistics were therefore used to analyze data. The Friedman test was used to compare multiple populations, and the Wilcox on test was used to compare two populations. The Bonferroni correction was applied for multiple comparisons. In these cases, the cutoff P value for significance (P=0.05) was divided by the number of comparisons to arrive at an adjusted P-value.
Results
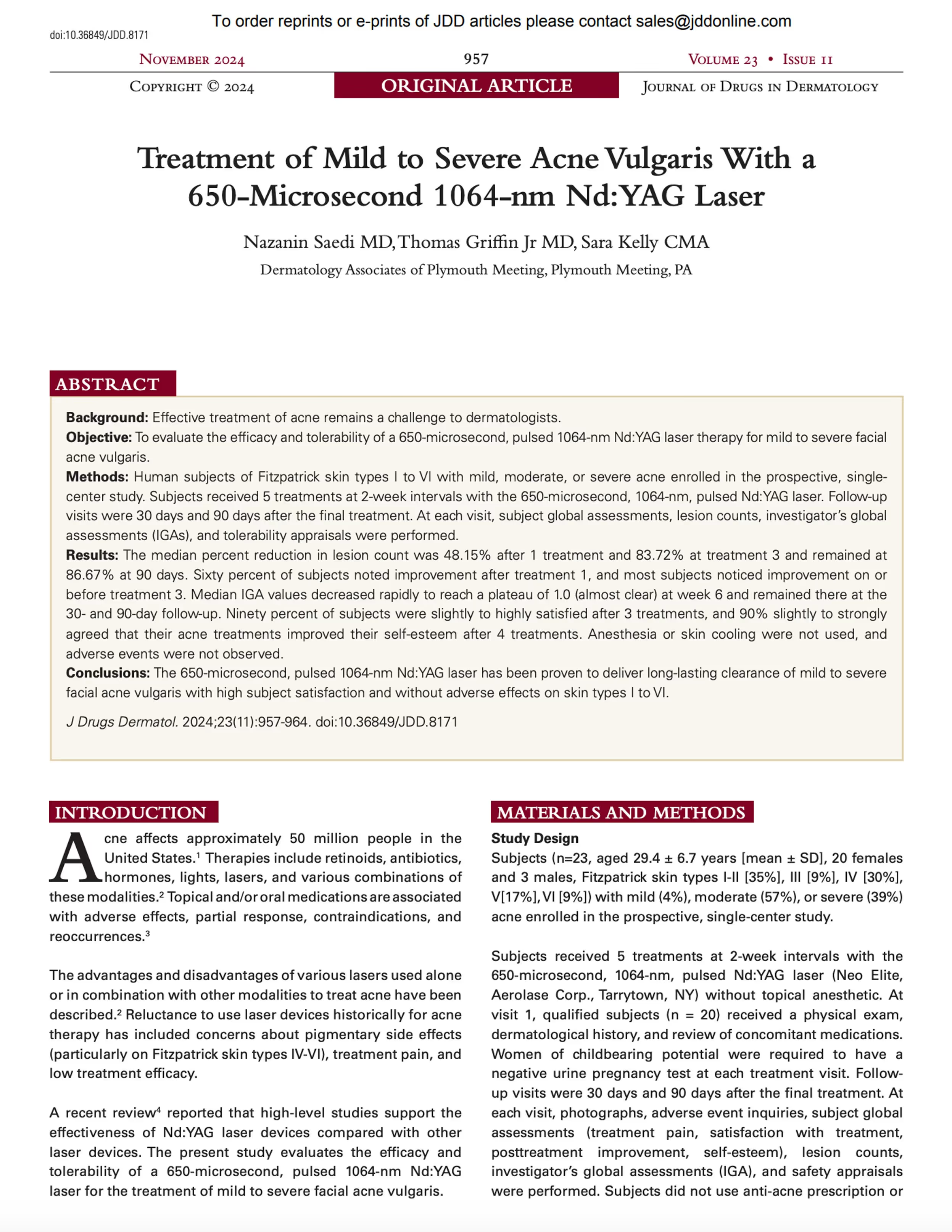
Twenty subjects completed the study. The data are shown in Table 3.
Acne Lesion Counts
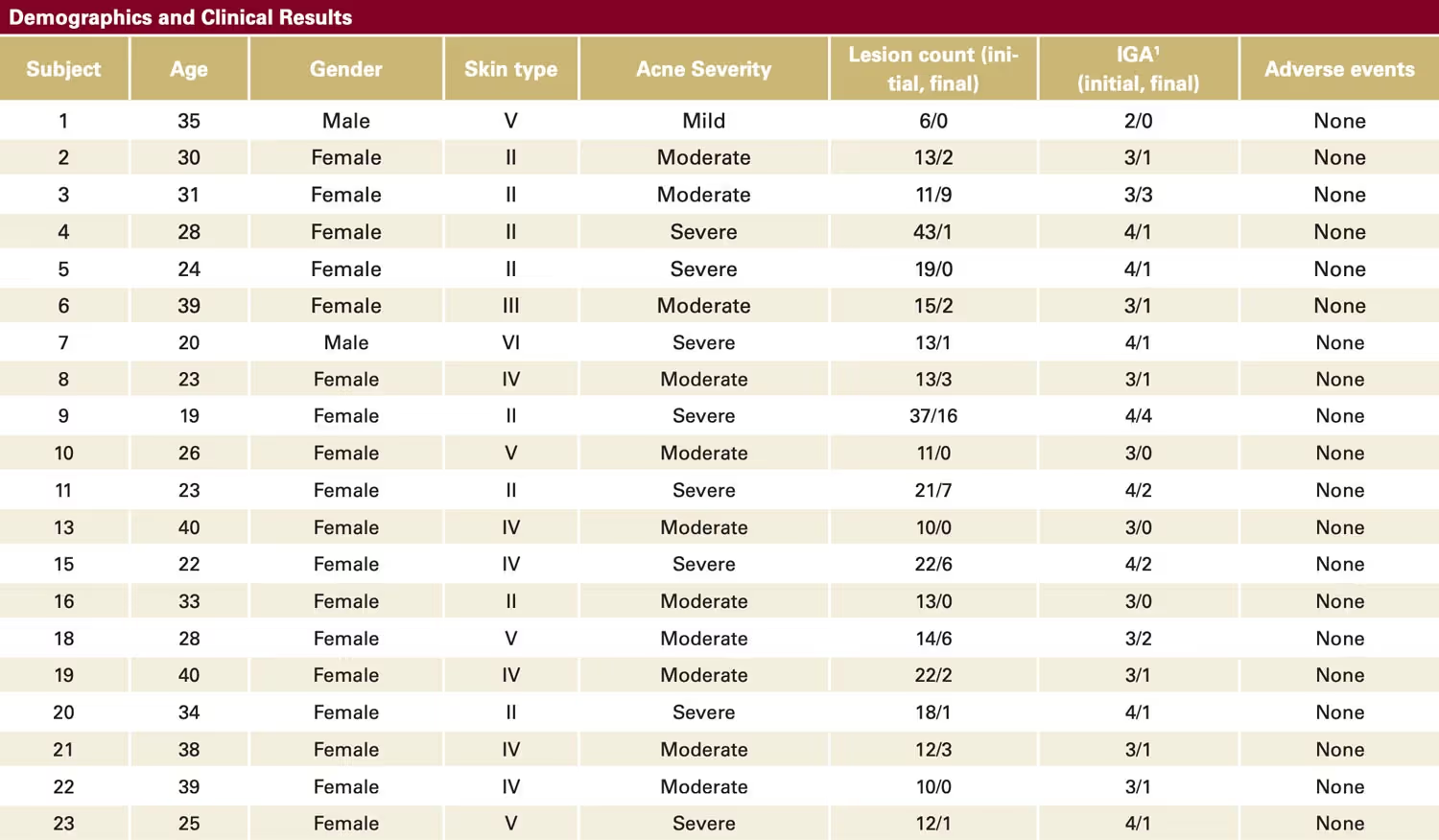
As shown in Figure 1, inflammatory acne lesions decreased rapidly by week 2 and continued to decrease throughout the study. The median inflammatory acne lesions decreased from13.5 to 7.0 by week 2 and to 1.5 at 90 days. The Wilcox on test was used to compare week 6 data and 90-day data with baseline. P-values were 0.0010 in both cases, which, when the Bonferroni correction was applied (P=0.025 as the cutoff value), was significant.
The median percent reduction in inflammatory lesion counts from baseline was calculated for week 6 and 90 days by the following formula:
% reduction = 100 x (count at week 6 or 90 days – counts at baseline)/count at baseline.
The median percent reduction in lesion count was 83.72% (range 36.36 to 100.00) at 6 weeks (after treatment 3) and 86.67% (range 18.18 to 100.00) at 90 days.
Six non-independent comparisons were made with baseline, and the Bonferroni-adjusted significance level was 0.05/6 = 0.0084.Decreases in counts compared to baseline were significant as early as week 2 (P<0.0001), a pattern that continued for the remainder of the study. Friedman’s test for week 6, week 8, 30days, and 90 days showed that the difference among the median lesion counts for these four populations was insignificant (P=0.1328), suggesting that lesion counts reach a minimum at week 6, after only 3 treatments, and that the reduced counts persisted for the remainder of the study.
Figure 1
Median acne lesion counts of subjects during the study period.
Discomfort During Treatment
The median discomfort was 2.0 for the first, second, and final treatments and 3.0 for the third and fourth treatments. Differences in median scores among treatments were not significant.
Percentage of Subjects Showing Improvement After a Specific Treatment Session
Subjects were asked to specify after which treatment, ie, 0 (baseline) to treatment 5, he or she first noticed an improvement in their acne. At week 6 (after treatment 2), 60% of subjects noted improvement after treatment 1, while an additional 35%, ie, a total of 95%, reported improvement after treatment 2.
Percent Clearance of Acne
The percentage clearance of acne was estimated by subjects after each treatment and at the 30-day follow-up visit. Clearance increased steadily throughout the study period and reached a median of 90% (30%-100%) at 30 days. All but 6 subjects achieved at least 80% clearance at 30 days.
Investigator’s Global Assessment
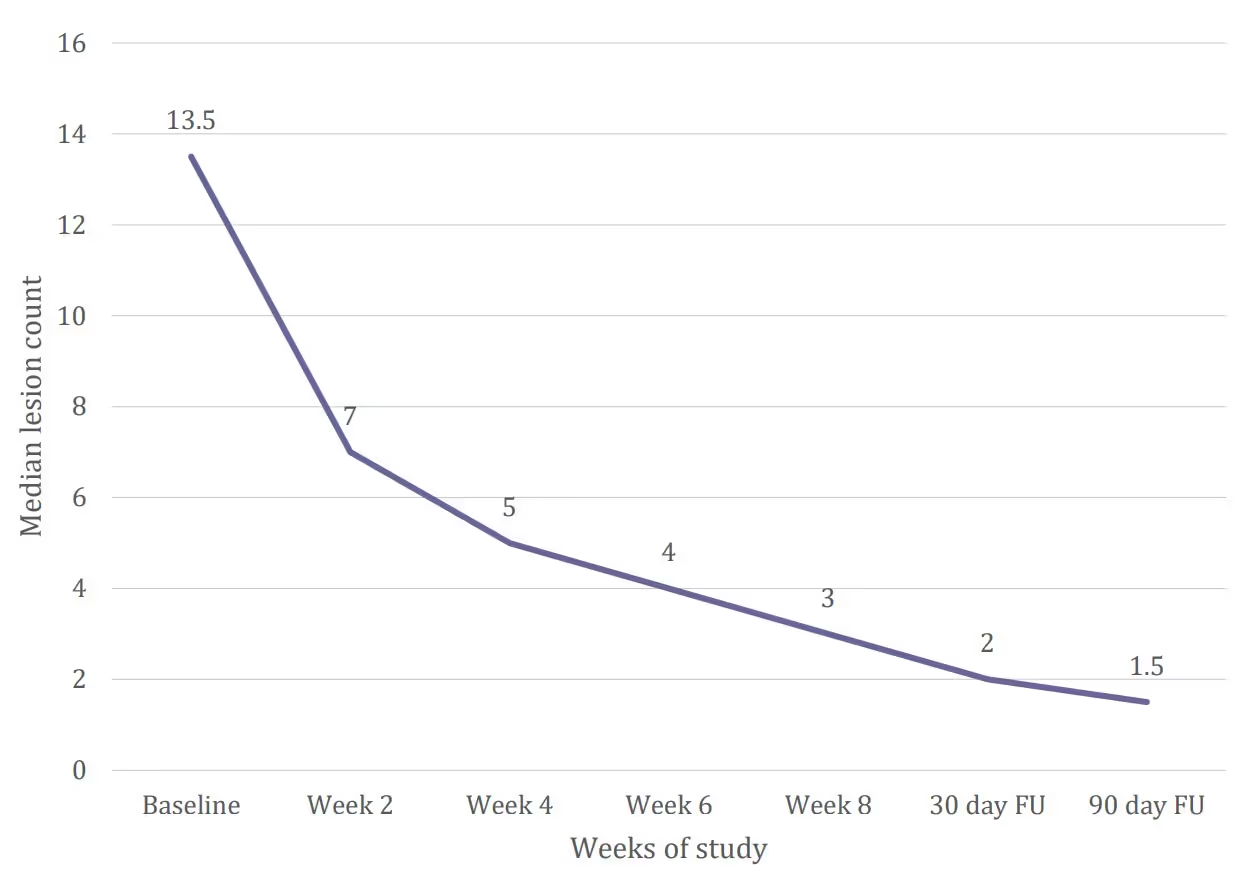
Figure 2 shows the median IGA values throughout the study period. Median values decreased rapidly and reached a plateau at week 6. These results were confirmed when subject scores at week 6, week 8, 30 days, and 90 days were compared by Friedman’s test. The P value of 0.1870 indicates that the median values of the 4 populations did not differ significantly. These results suggest that most subjects achieved noticeable clearance by week 6, after 3 treatments, and that clearance persisted for up to 90 days.
Figure 2
Median Investigator’s Global Assessment (IGA) scores of subjects during the study period.
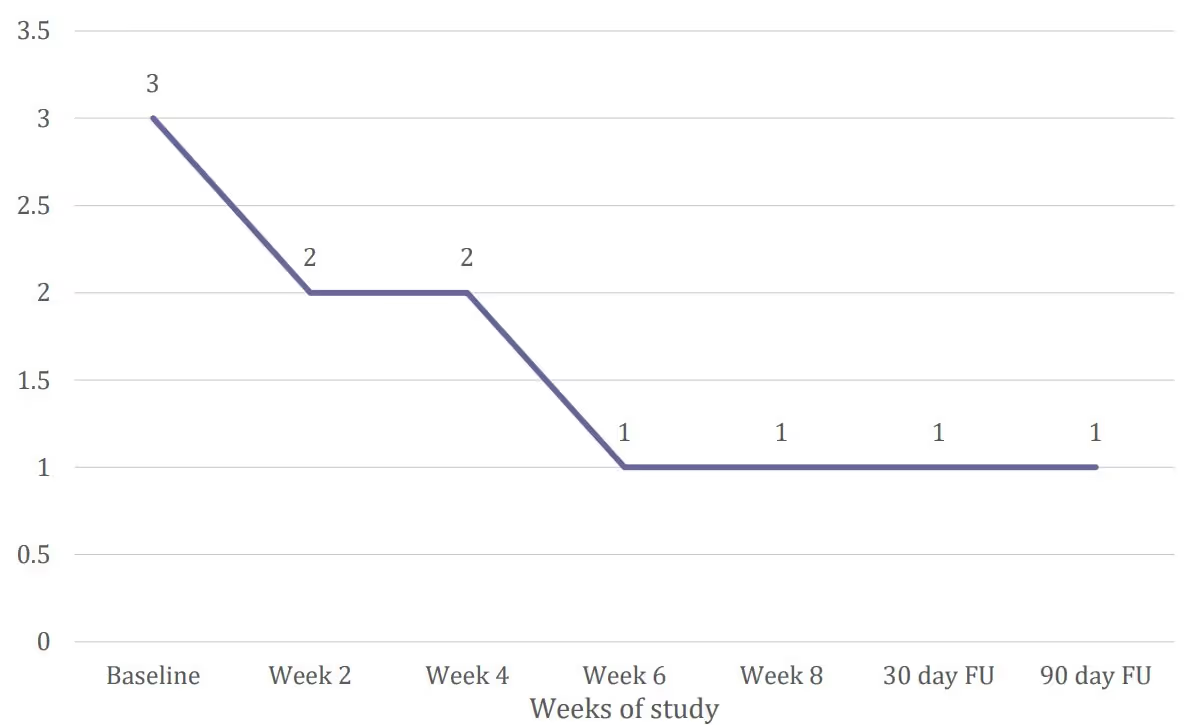
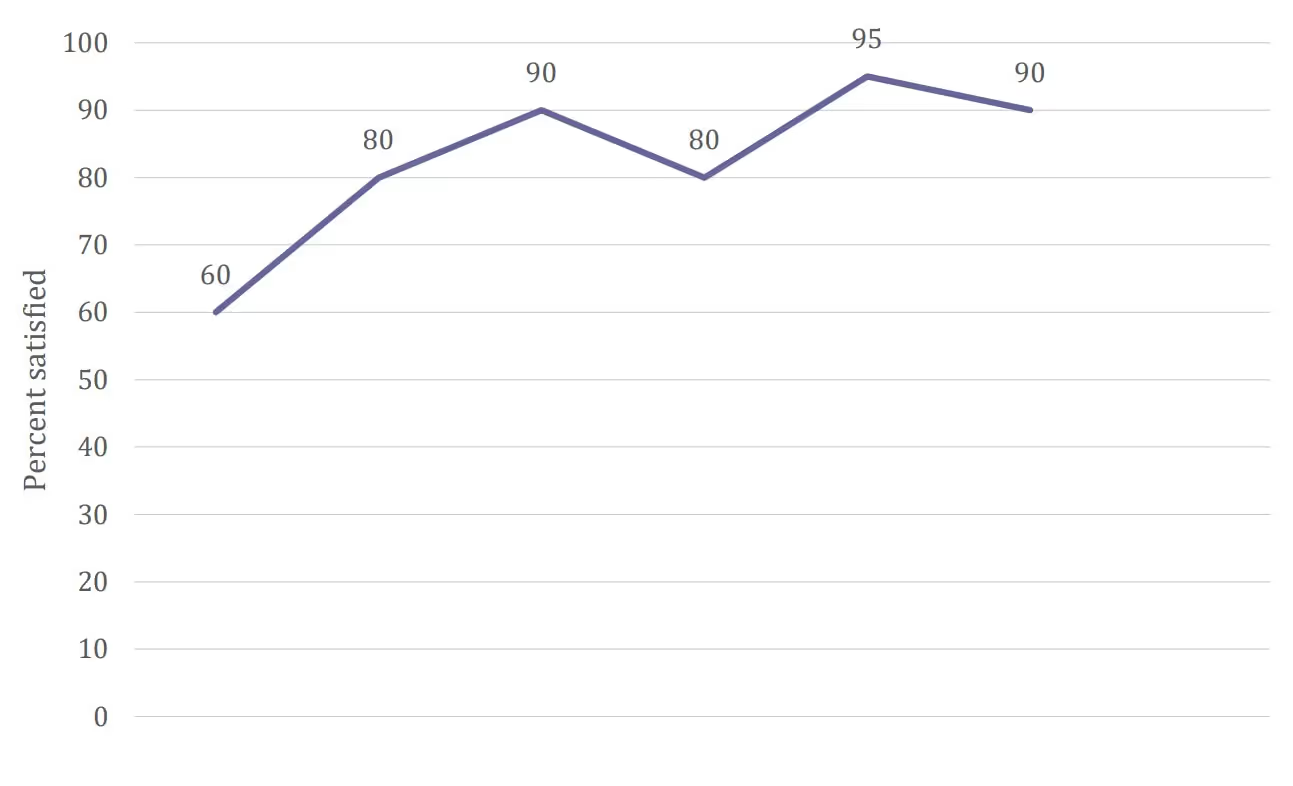
Figure 3
Percentage of subjects slightly to highly satisfied (4 to 5) with treatment during the study period.
The Wilcoxon test was used to compare week 6 data and 90-day data with baseline. P-values were <0.0001 in both cases, which, when the Bonferroni correction was applied (P=0.025 as the cutoff value), was significant. The median percent reduction in IGA score was 66.67% (range 0.00 to 100.00) at both 6 weeks and 90 days.
Satisfaction With Treatment
Figure 3 shows steadily increasing satisfaction with treatment; 90% of subjects were slightly to highly satisfied by the 90-day follow-up. Comparison of satisfaction at week 6 (after 3 treatments) through 90 days by Friedman’s test revealed a P value of 0.7182, confirming that the median values of the 4 populations (5.0 at week 6, 4.5 at week 8, 4.5 at 30 days, and 5.0 at 90 days) did not differ significantly. This suggests that most subjects achieved satisfaction by week 6 (after 3 treatments), and that satisfaction persisted for the remainder of the study.
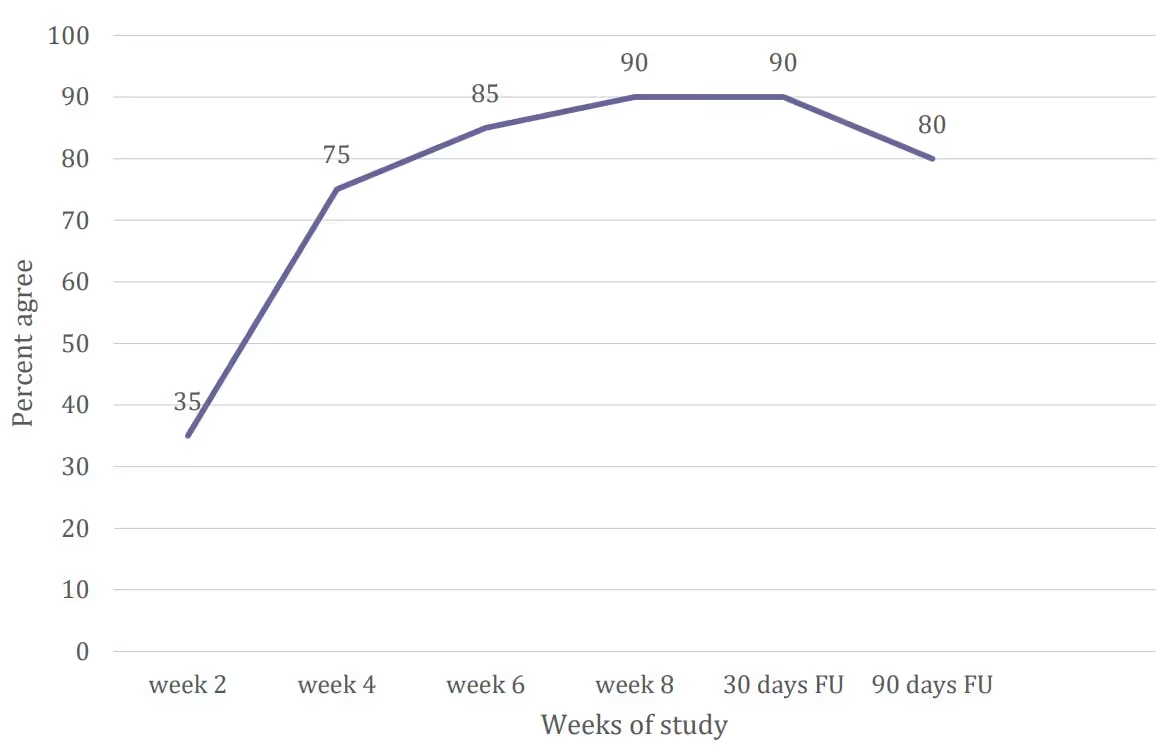
Self-Esteem
Figure 4 shows the percentage of subjects that agree that their acne treatments have improved their self-esteem at each time point. Self-esteem increased during the study with peaks at week 8 and 30 days. Friedman’s test for week 6, week 8, 30 days, and 90 days yielded a p value of 0.6861, indicating that the medians of the 4 populations (4.0, 5.0, 4.0, 5.0, respectively) did not differ significantly. The minimum and maximum values were 3 and 5, respectively, for each population. These results suggest that most subjects achieve improved self-esteem by week 6, after 3 treatments, and that self-esteem persisted through the rest of the study.
Figure 4
Percentage of subjects slightly to strongly agree (4 to 5) that their acne treatments have improved their self-esteem during the studyperiod.
Adverse Events
Edema, erythema, acne flare-ups, dryness, and itchiness on ascale of none, mild, moderate, or severe were not observed during the study. Clinical examples are shown in Figures 5 through 8.




Discussion
The results show that clinically meaningful results in acne lesion counts, subjective improvement, IGA values, satisfaction with treatment, and self-esteem are obtained for subjects with a wide range of skin types (ie, Fitzpatrick I-VI) in 3 to 5 treatments with the 650-microsecond, 1064-nm, pulsed Nd:YAG laser. Edema, erythema, acne flare-ups, dryness, and itchiness were not observed. Subjects reported minimum discomfort with no anesthetic or skin cooling. The 650-microsecond 1064-nm Nd: YAG laser is a recent development for the treatment of acne. In a study by Khatri and colleagues,5 100 patients (aged less than 25 years, skin types II to III) with moderate to severe acne received three treatments at 1-week intervals with the 650-microsecond laser. For inflammatory lesions, treatment settings were similar to those of the present study. Anesthetic or pre-cooling were not used, and pain was minimal during and after treatment. Patient satisfaction was high and hyperpigmentation, burns, scars, and other adverse effects were not observed. In a clinical evaluation of acne treatment using the 650-microsecond pulsed Nd:YAG 1064-nm laser,6 all patients noted improvement of their acne as early as 2 weeks after their first treatment. Several patients also experienced lightening of post-inflammatory hyperpigmentation and all patients noticed an overall reduction in larger cystic and inflammatory lesions. They reported a well-tolerated procedure without complications or downtime.
Kesty and Goldberg,7 in a randomized, sham-controlled study, reported the efficacy of the 650-microsecond laser in the treatment of 20 subjects (aged 12 to 40 years, skin types I to VI) with moderate to severe facial acne. As in the present study, treatment settings varied with Fitzpatrick skin type. All subjects received 3 treatments at 2-week intervals and an additional treatment 4 weeks later, all with either the laser or sham control.For the laser-treated group, IGA improvement was 26% compared with 7% for the sham group and the number of inflammatory lesions decreased by 42% vs 26% for the sham group. The laser-treated subjects achieved a reduced total number of comedones, a lower total porphyrin score, and an18% reduction in sebum production. With this study by Kesty and colleagues the reduction in lesion count and IGA score was not as dramatic as with the present study, which indicates that the method of the current study of 5 laser treatments every two weeks delivers higher rates of reduction in lesion count.
In the present study, the median percent reduction in IGA score was 66.67% at both 6 weeks (after 3 treatments) and 90 days (after 5 treatments) and the median percent reduction in lesion count was 83.72% at 6 weeks and 86.67% at 90 days.The differences from the results of Kesty and colleagues may be attributed to different treatment methods used, both in number of treatments and interval between treatments.The present study used 5 treatments at bi-weekly intervals, versus 3 treatments at bi-weekly intervals followed by a fourth treatment after a 4-week pause in Kesty and colleagues. Another difference was the expression of Kesty and colleagues’ IGA and lesion count results as mean values rather than median values. The 5 biweekly treatment protocol was proven to be optimal to maximize the acne clearance effectiveness and long-term results.
When used to treat acne, the 650-microsecond 1064-nm laser energy is clinically proven to reduce sebum output,7 thus reducing a key component of the pathogenesis of acne. One hypothesis is that this laser’s effect of coagulating small capillaries in the skin tissue8 may be a contributing factor to the reduction of output of sebaceous glands. Regardless of the exact mechanism of action, suppressing sebum output without actually destroying sebaceous glands can be advantageous since sebum production is critical for maintaining skin homeostasis, lubrication, and physiological defense against environmental and infectious insults.9,10
Isotretinoin is a common systemic therapy for active acne, and the question often arises regarding whether laser therapy can be performed on a patient who is being treated with this medication. In a study by Gold and colleagues,11 46 patients(aged 18 to 30 years, skin types I to III) with moderate to severe acne received a combination therapy of systemic isotretinoin at a low dosage (0.2-0.3 mg/kg/day) and 12 facial laser treatments at 2-week intervals with the 650-microsecond laser at 21 J/cm2. All patients completed the study. IGA reduction was 72.2% and Dermatology Life Quality Index reduction was 72.3%. Inflammatory elements resolved without scarring and without adverse effects.
Traditional 1064-nm lasers often use pulse durations of 5 to 30 milliseconds, which are well in excess of the thermal relaxation time (TRT) of skin tissue, which is approximately 0.8 milliseconds. With these ultra-long pulse durations, the skin must be cooled continuously during treatment with gels, sprays and/or contact cooling plates. Additionally, in spite of the cooling, treatment with these traditional lasers can still be very painful. This new 1064-nm laser technology with a 650-microsecond pulse duration treats the skin beneath its TRT, negating the need for numbing and skin cooling and enabling uniquely gentle, sanitary and effective laser treatment experiences for patients of color.12 In addition to the skin type versatility of this laser it has also shown to be safe and efficacious for other indications such as permanent hair reduction, hyperpigmentation, melasma and onychomycosis.5,13,14-17 Limitations of the study include the relatively short 90-days post treatment follow-up time and the absence of a control group.
Conclusion
The 650-microsecond, pulsed 1064-nm Nd:YAG laser has been shown to improve mild to severe acne vulgaris with high subject satisfaction and without adverse effects.
Disclosures
Dr Saedi is a consultant for Aerolase. Dr Griffin and Sara Kelly have no conflicts of interest to disclose.
References
- Barbieri JS, Spaccarelli N, Margolis DJ, et al. Approaches to limit systemic antibiotic use in acne: systemic alternatives, emerging topical therapies, dietary modification, and laser and light-based treatments. J Am Acad Dermatol. 2019;80:538-549.
- Gold MH, Goldberg DJ, Nestor MS. Current treatments of acne:medications, lights, lasers, and a novel 650-μs 1064-nm Nd: YAG laser.J Cosmet Dermatol. 2017;16:303-318.
- Keyal U, Bhatta AK, Wang XL. Photodynamic therapy for the treatment of different severity of acne: A systematic review. Photodiagnosis Photodyn Ther. 2016;14:191-199.
- Li MK, Liu C, Hsu JTS. The use of lasers and light devices in acne management: an update. Am J Clin Dermatol. 2021;22:785-800.
- Khatri KA, Lee RA, Goldberg LJ,, et al. Efficacy and safety of a 0.65millisecond pulsed portable ND: YAG laser for hair removal. J Cosmet LaserTher. 2009;11:19-24.
- Greywal T, Ortiz A. 1064nm Nd:YAG laser with a 650-microsecond pulse duration for the treatment of acne: a clinical evaluation. Presented at the annual conference of the American Society of Laser Medicine and Surgery,Phoenix, AZ, April 29-May 3, 2020.
- Kesty K, Goldberg DJ. 650 usec 1064nm Nd:YAG laser treatment of acne: A double-blind randomized control study. J Cosmet Dermatol. 2020;19:2295-2300.
- Rose AE, Goldberg DJ. Successful treatment of facial telangiectasias using a MicroPulse 1,064-nm neodymium-doped yttrium aluminum garnet laser. Dermatol Surg. 2013;39:1062-1066.
- Zouboulis CC. [The sebaceous gland]. Hautarzt. 2010;61:467-468,4704,476-477.
- Picardo M, Mastrofrancesco A, Bíró T. Sebaceous gland-a major player in skin homoeostasis. Exp Dermatol. 2015;24:485-486.
- Gold MH, Manturova NE, Kruglova LS, et al. Treatment of moderate to severe acne and scars with a 650-microsecond 1064-nm laser and isotretinoin. J Drugs Dermatol. 2020;19:646-651.
- Cook-Bolden F. A novel 0.65 millisecond pulsed 1064 nm laser to treat skin of color without skin cooling or anesthetics. J Drugs Dermatol. 2011;10(12Suppl):s10-s11.
- Hochman LG. Laser treatment of onychomycosis using a novel0.65-millisecond pulsed Nd:YAG 1064-nm laser. J Cosmet Laser Ther.2011;13:2-5.
- Giambrone D, Ahn C, Rao B. Laser hair removal using a 650 microsecond pulsed ND:YAG laser: a study of 298 patients. J Glob Dermatol. 2014;1:9-12.
- Henry M. Treatment of hyperpigmentation on skin of color using a 650-microsecond pulsed 1064nm Laser. Poster presented at the annual meeting of the American Society of Dermatologic Surgery, Phoenix, AZ, October 11-14, 2018.
- Greywal T, Ortiz A. Treating melasma with the 1064 nm Nd:YAG laser with a 650-microsecond pulse duration: A clinical evaluation. J Cosmet Dermatol. 2021;20:3889-3892.
- Pinski K, Mannausa K. Comprehensive non-ablative laser skin rejuvenation using a novel 650 microsecond pulsed Nd: YAG 1064-nm laser. Lasers SurgMed. 2017; 49:417-467, E77.

Treatment of Acne Vulgaris With a 650-microsecond, 1064nm Nd:YAG Laser: A Retrospective Study
This clinical article aims to evaluate the efficacy and tolerability of a 650-microsecond laser for the treatment of mild to severe facial acne vulgaris.
Current Treatments of Acne: Medications, Lights, Lasers, and a Novel 650-Microsecond 1064nm Nd: YAG Laser
The purpose of this study was to review current therapies for acne of all severities and to introduce the 650-microsecond 1064-nm laser for the treatment of acne.

650-microsecond 1064nm Nd:YAG laser treatment of acne: A double-blind randomized control study
Laser therapy can be successful in diminishing acne vulgaris lesions by halting overactive sebaceous gland activity and alleviating the effects of inflammation.